Sinus headache vs migraine: how to tell the difference (ENT specialist guide)
Most people who think they have a 'sinus headache' actually have migraine. A clear ENT specialist guide to telling the two apart—so you stop chasing antibiotics for a problem that needs a different treatment.

If you have been treated for “sinus headaches” repeatedly—courses of antibiotics, decongestants, nasal sprays, steam inhalation—and the headaches still keep coming back, there is a strong chance the real diagnosis is migraine, not sinusitis.
This is one of the most common, and most consequential, diagnostic confusions in ENT practice. Multiple international studies have shown that the majority of patients who present believing they have a “sinus headache” actually meet criteria for migraine. The symptoms genuinely overlap—facial pressure, forehead pain, blocked nose, watery eyes—and that is why the mistake is so easy to make.
This guide, written from clinical experience at Dr Joel’s Clear ENT Clinic in Thiruvananthapuram, walks through the difference between sinus headache vs migraine, why migraine so often masquerades as a sinus problem, and how an ENT specialist sorts the two out without unnecessary scans or antibiotics.
The single most useful thing to know is this: if your headaches keep coming back even though every sinus treatment has been tried, the diagnosis itself is probably wrong.
What is a sinus headache?
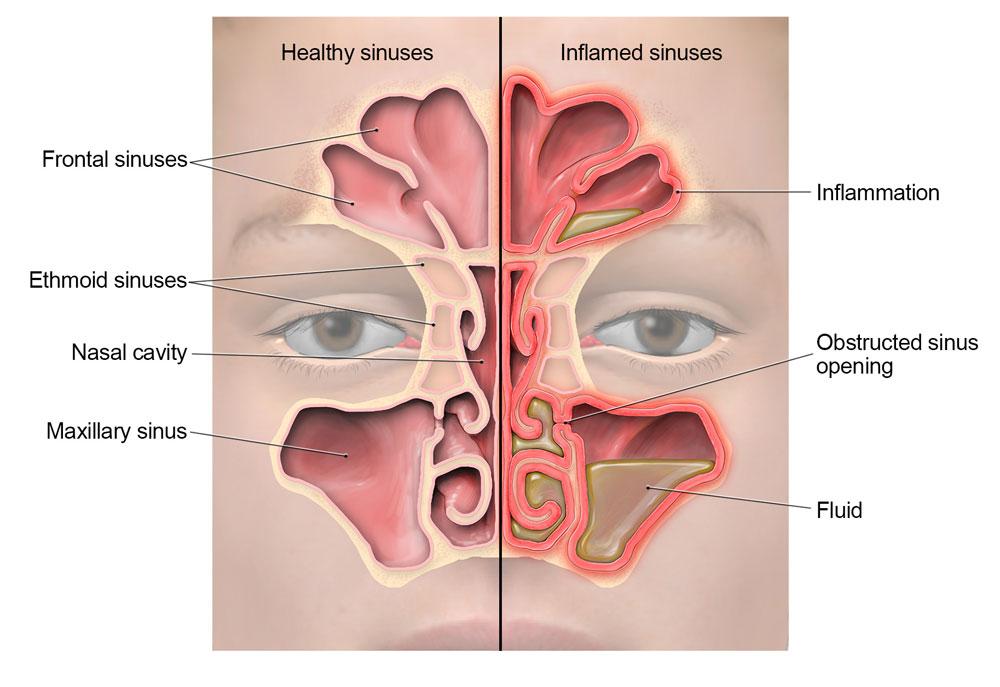
A true sinus headache is a headache caused by inflammation or infection of the paranasal sinuses—the air-filled cavities behind the cheeks (maxillary), between the eyes (ethmoid), in the forehead (frontal), and deep behind the nose (sphenoid).
When the natural drainage pathways of these sinuses become blocked—by a viral cold, allergy, or a polyp—mucus and pressure build up inside, the lining becomes inflamed, and pain is felt over the affected sinus.
Common underlying causes include:
- Acute viral or bacterial sinusitis.
- Chronic sinusitis lasting more than 12 weeks.
- Allergic rhinitis with sinus involvement.
- Nasal polyps blocking sinus drainage.
- A deviated nasal septum contributing to obstruction.
A genuine sinus headache almost always has objective signs of sinus disease, not just facial pain. That is the key.
What is a migraine?
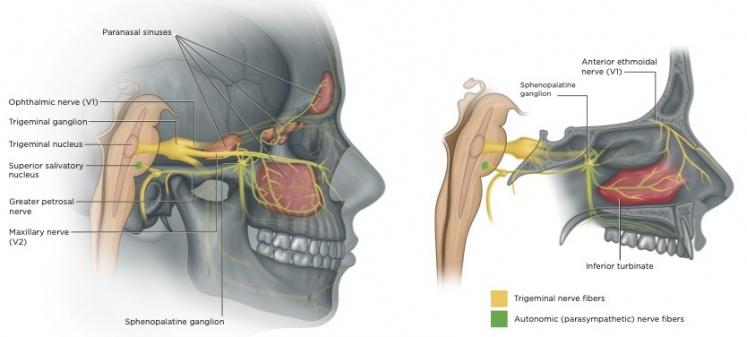
Migraine is a neurological disorder, not “just a bad headache”. It involves abnormal sensitivity of certain nerves and brain pathways, particularly the trigeminal system, which supplies the face, forehead, eyes, and nose.
Because the trigeminal nerve serves both the face and the lining of the nose and sinuses, a migraine attack frequently produces:
- Throbbing or pulsating head pain (often, but not always, one-sided).
- Facial pressure and forehead heaviness.
- Nasal congestion and even a runny nose.
- Watery eyes and pressure around or behind the eye.
- Nausea, sometimes vomiting.
- Sensitivity to light and sound.
- Worsening with movement or bending forward.
Read that list again. Almost every “classic” sinus symptom is on it. That is precisely why migraine is so often mistaken for sinus disease, and why patients who really have migraine end up taking course after course of antibiotics with no benefit.

The scene above is typical of how a migraine attack actually presents in real life: a sudden, throbbing one-sided head pain in a noisy, brightly-lit environment, with the patient instinctively pressing the temple and needing to retreat from light and sound. None of this points to the sinuses—it points to migraine.
The single most important medical fact
In multiple well-conducted studies, when patients who self-diagnosed with “sinus headache” were carefully evaluated, the majority were actually found to have migraine, with no evidence of sinus infection on examination or imaging.
This means that for many patients, repeated antibiotics, nasal sprays, or sinus treatments simply will not solve the real problem—because the real problem is not in the sinuses at all.
Sinus headache vs migraine: the key differences
The two conditions can be distinguished by paying attention to five things: location of pain, nature of pain, associated symptoms, duration, and triggers.
1. Location of pain
Sinus headache:
- Centred over the cheeks, forehead, between the eyes, or above the upper teeth.
- Often bilateral (both sides), tracking the affected sinus.
- Worse on bending forward, coughing, or straining.
Migraine:
- Often one-sided, but can affect both sides.
- Felt at the temple, behind the eye, the forehead, or even the cheek.
- Can mimic sinus pressure exactly—including pain that worsens on bending forward.
The takeaway: location alone does not reliably tell the two apart. Both can sit over the cheeks and forehead.
2. Nature of pain
Sinus headache:
- Pressure, heaviness, fullness.
- Steady rather than pulsating.
- Often described as “weight on the face”.
Migraine:
- Throbbing or pulsating, often in time with the heartbeat.
- Moderate to severe intensity.
- Worsened by routine activity such as walking up stairs.
A throbbing, movement-sensitive headache is a strong clue for migraine, even if the patient is convinced it is “sinus”.
3. Associated symptoms
This is where the diagnosis usually becomes clear.
True sinusitis often includes:
- Thick yellow or green nasal discharge.
- Fever (especially in acute bacterial sinusitis).
- Reduced sense of smell.
- Tenderness when pressing on the cheek or forehead.
- A recent viral cold that became worse instead of better.
- Symptoms lasting more than 10 days, or worsening after initial improvement.
Migraine often includes:
- Nausea, sometimes vomiting.
- Sensitivity to light (photophobia) and sound (phonophobia).
- Need to lie down in a dark, quiet room.
- Worsening with movement.
- Visual disturbances (zig-zag lines, flashing) before the headache—classical aura, not always present.
- A history of similar attacks over months or years, with normal periods in between.
A patient who repeatedly says “I had to switch off the lights and lie down” is describing migraine, not sinusitis.
4. Duration and pattern
Sinus headache:
- Tied to an active episode of sinus inflammation.
- Builds over days, often with a recent cold.
- Improves as the sinus infection resolves.
- May persist longer in chronic sinusitis, but with continuous nasal symptoms.
Migraine:
- Discrete attacks lasting 4 to 72 hours.
- Recur over months or years with headache-free periods in between.
- Patients can often describe their attacks: “I get this every 2–3 weeks for the past 5 years.”
If the headache pattern is “comes and goes for years, with completely normal weeks in between”, it is almost never sinusitis.
5. Triggers
Sinus headache:
- Viral colds.
- Allergy flares.
- Sometimes weather/humidity changes.
Migraine:
- Stress and stress let-down (weekend headaches).
- Lack of sleep, or sleeping too long.
- Skipping meals or dehydration.
- Certain foods (chocolate, aged cheese, MSG, alcohol).
- Bright light, strong smells, hormonal changes.
- Travel and screen time.
A headache reliably triggered by missed meals or poor sleep is a migraine until proven otherwise.
Why migraine produces “sinus symptoms”
This is the part most patients have never had explained to them, and once they understand it, the whole picture clicks into place.
A migraine attack activates branches of the trigeminal nerve, which not only carries pain from the face but also controls reflexes in the nasal lining. When migraine fires, those reflexes can produce:
- Nasal congestion and a feeling of blockage.
- Clear watery discharge.
- Watering and redness of the eye.
- Pressure around the eyes and forehead.
- Tenderness over the cheekbones.
To the patient, this feels exactly like a sinus problem. To the body, it is a neurological event with a nasal “side effect”. This is why sinus pressure and nasal symptoms during a migraine do not mean you have sinusitis—and why CT scans in these patients are usually normal.
When sinus disease really is the cause
Lean toward a true sinus headache if you have:
- Thick coloured (yellow/green) nasal discharge.
- Fever.
- A recent cold that became worse, not better, after a few days.
- A persistently blocked nose lasting weeks.
- Reduced or lost sense of smell.
- Tenderness over the cheek or forehead on examination.
- Improvement with proper sinus treatment that holds up over time.
These objective features point to inflammation in the sinuses themselves, not a neurological process.
When migraine is more likely
Lean toward migraine if you have:
- Recurrent headaches over months or years, with normal periods in between.
- Throbbing or pulsating pain.
- Nausea, photophobia, or phonophobia.
- A reliable trigger pattern (sleep, stress, missed meals).
- A family history of migraine.
- Previous CT scans of the sinuses that were reported as normal.
- No improvement despite multiple courses of antibiotics and nasal sprays.
The last point alone—repeated sinus treatment without lasting relief—is one of the strongest clues that the diagnosis itself needs revisiting.
How an ENT specialist evaluates this properly

At Dr Joel’s Clear ENT Clinic in Thiruvananthapuram, evaluation of a suspected “sinus headache” is structured to answer one question first: is there actually anything wrong with the sinuses, or not? A large part of the consultation is spent simply explaining the anatomy and the difference between sinus disease and migraine, because once a patient understands why their facial symptoms are not coming from the sinuses, the next steps make sense.
A typical assessment includes:
- A focused history — pattern, duration, triggers, associated symptoms, response to previous treatment.
- Anterior rhinoscopy — direct examination of the front of the nose for swelling, polyps, or septal issues.
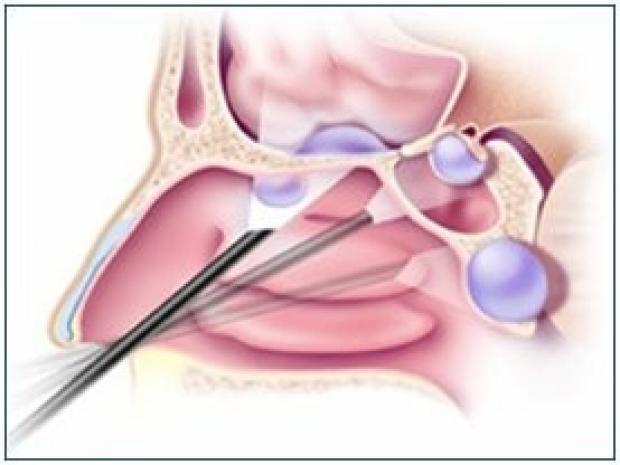
- Diagnostic nasal endoscopy — a painless, in-office examination that lets us look at the deeper drainage pathways of the sinuses with a thin scope. This is the single most useful bedside test in this scenario.
- Allergy assessment when relevant.
- CT scan only when indicated — for example, suspected chronic sinusitis, polyps, or before sinus surgery. CT is not a screening test for headache.
- Onward migraine care — if the picture clearly points to migraine, we explain the diagnosis and either guide initial migraine management or refer to a neurologist for advanced care.
The aim is to give the patient a clear answer, not a never-ending cycle of partial treatments.
Treatment is very different for the two conditions
This is why the diagnosis matters so much—the correct treatment depends entirely on the correct label.
If it is sinusitis
- Saline nasal rinses (large-volume isotonic saline) — often underrated, but very effective.
- Intranasal steroid sprays — the mainstay of medical management for chronic and allergic sinusitis.
- Allergy treatment — antihistamines or specific therapy when allergy is driving the inflammation.
- Antibiotics — only when there is a clear bacterial picture (high fever, severe symptoms, worsening after a viral cold), not for every facial pressure complaint.
- Surgery (FESS) — reserved for selected cases of chronic sinusitis or polyps that do not respond to medical therapy.

If it is migraine
- Trigger identification and lifestyle modification — sleep, hydration, regular meals.
- Acute (abortive) treatment — taken at the first sign of an attack.
- Preventive treatment — daily medication when attacks are frequent or disabling.
- Stress and screen-time management.
Using sinus antibiotics for migraine, or migraine medication for true bacterial sinusitis, will both fail. That is why labelling the condition correctly is the most important step.
Common patient mistakes seen in Kerala
These observations are made gently, not as criticism—they are simply the patterns we see most often in clinic:
- Repeated antibiotic courses from pharmacies for any “sinus headache”, without examination.
- Relying on steam inhalation alone for years, without ever finding out what is actually inflamed.
- Random over-the-counter combinations of decongestants and painkillers, taken so often that they cause medication-overuse headache—which itself perpetuates the problem.
- Believing that any pain over the cheeks must be sinusitis, and rejecting a migraine diagnosis as “just a headache”.
- Postponing ENT consultation until the headaches have already disrupted work and sleep for years.
- Insisting on a CT scan as the first step, when nasal endoscopy in clinic would have answered the question more accurately.
A single, well-structured ENT consultation can usually settle the question of sinus headache vs migraine in one visit, and redirect treatment to whatever actually works for that patient.
When to seek urgent medical help
Most sinus headaches and migraines are not dangerous. However, certain features mean the headache needs emergency evaluation, not an outpatient appointment:
- A sudden, severe “worst headache of life”.
- Headache with weakness, numbness, slurred speech, or facial droop.
- Headache with vision loss or double vision.
- Headache with confusion or altered consciousness.
- Headache with high fever and neck stiffness.
- Persistent vomiting that prevents fluid intake.
- A new severe headache after a head injury.
- A new persistent headache pattern in someone over 50, or in someone with cancer or a weakened immune system.
If any of these are present, go to an emergency department directly.
Key takeaway
If you have been treated repeatedly for “sinus headaches” without lasting relief, the diagnosis itself needs to be reconsidered. The most likely alternative is migraine, which behaves like a sinus problem because of how the trigeminal nerve is wired—but needs an entirely different treatment plan.
To recap:
- A true sinus headache almost always has objective signs of sinus disease—coloured discharge, reduced smell, fever, or findings on examination.
- Migraine often produces facial pressure, nasal congestion, and watery eyes, which is why it is so often misdiagnosed as sinusitis.
- Throbbing pain, light/sound sensitivity, nausea, and a years-long pattern of attacks point strongly to migraine.
- Most patients do not need repeated CT scans—nasal endoscopy in the clinic is more useful.
- Antibiotics for a headache that is actually migraine will keep failing.
If you or a family member has been searching for an ENT for sinus headache, struggling with chronic facial pain, sinus pressure, or recurring forehead headaches, an early, focused evaluation at Dr Joel’s Clear ENT Clinic in Thiruvananthapuram can usually give you a clear answer—and stop years of treatment in the wrong direction.

