Snoring and obstructive sleep apnea: when snoring becomes a serious health risk
Loud habitual snoring can be a warning sign of obstructive sleep apnea—a treatable condition linked to high blood pressure, heart disease, stroke, diabetes, and accidents. An ENT specialist guide to when snoring is serious.

Snoring is often dismissed as a harmless nuisance or a family joke. But in many adults, loud habitual snoring is a warning sign of obstructive sleep apnea (OSA)—a treatable medical condition with strong, well-established links to high blood pressure, heart disease, stroke, diabetes, road traffic accidents, and reduced life expectancy.
If you or your partner snores loudly, gasps in sleep, or feels exhausted despite a full night in bed, this is not something to keep ignoring.
This guide, written from clinical practice at Dr Joel’s Clear ENT Clinic in Thiruvananthapuram, explains what snoring really is, when it crosses over into sleep apnea, why untreated OSA matters, how it is diagnosed, and what modern treatment looks like for patients in Trivandrum and across Kerala.
The single most important fact: snoring is a sound. Sleep apnea is a disease. Many people have one without the other—but loud, habitual snoring with daytime symptoms should always be evaluated.
What is snoring?
Snoring is the sound made when air is forced through a partially narrowed upper airway during sleep, causing the soft tissues of the throat—the soft palate, uvula, tongue base, and pharyngeal walls—to vibrate.
When you fall asleep, the muscles that keep your airway open relax. In some people, that relaxation is enough to narrow the airway and produce vibration; in others, it is enough to close the airway altogether—and that is sleep apnea.
Common contributors to snoring include:
- Nasal obstruction — deviated septum, allergic rhinitis, polyps, chronic sinusitis.
- Enlarged tonsils or a long, low-hanging soft palate and uvula.
- Tongue base prominence or retropositioned jaw (small or set-back lower jaw).
- Obesity, especially with a large neck circumference.
- Alcohol before bed and sedative medications.
- Sleeping on the back (gravity worsens airway collapse).
- Nasal congestion from any cause—including a simple cold.
Not all snoring means sleep apnea. But most people with OSA snore, and that is why snoring is the symptom that brings the diagnosis to attention.
What is obstructive sleep apnea (OSA)?
In OSA, the upper airway does not just narrow—it repeatedly collapses during sleep. Each collapse is an apnea (full stop in airflow) or hypopnea (significant reduction in airflow), typically lasting 10 seconds or more.
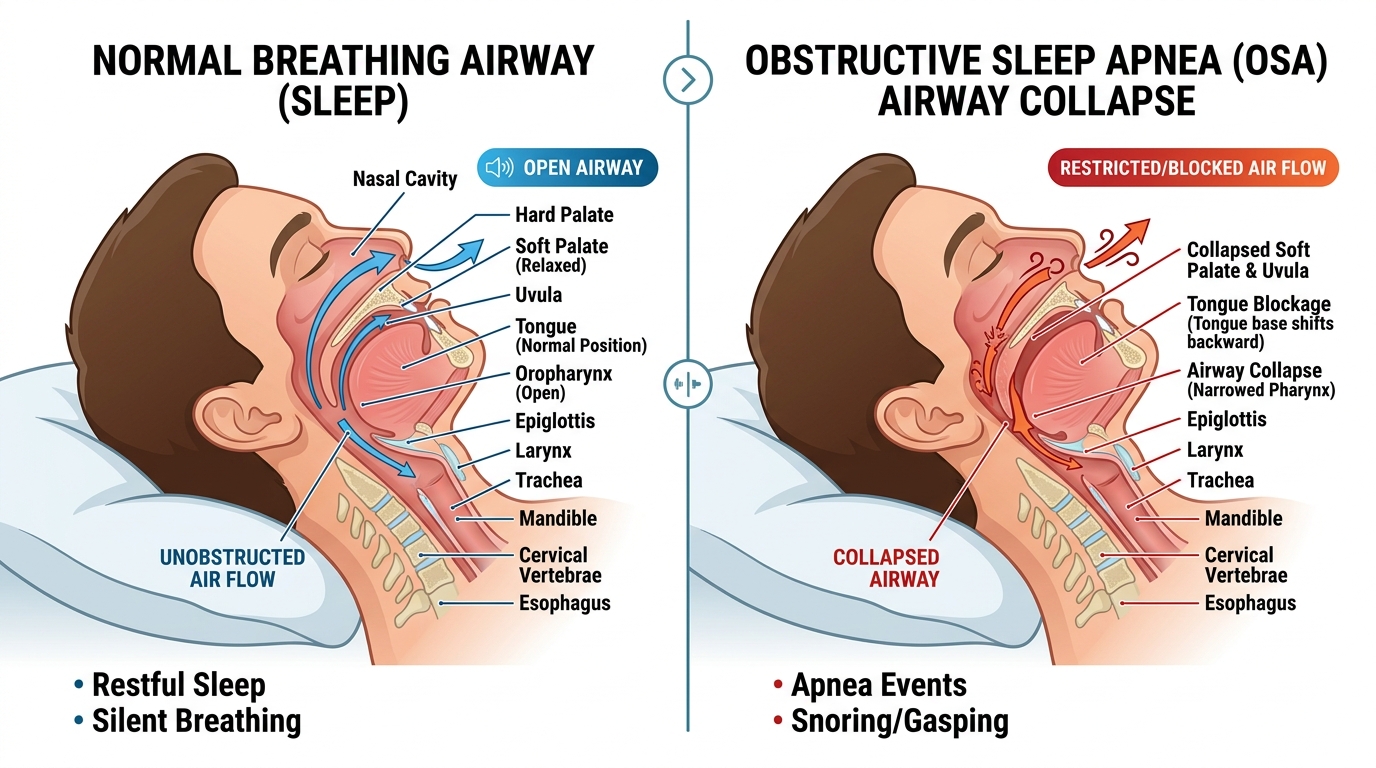
The diagram above shows what is happening anatomically. On the left, the airway is open and air flows freely; on the right, in OSA, the soft palate and uvula collapse backwards, the tongue base shifts back, and the pharynx narrows—blocking airflow even though the patient is still trying to breathe.
These episodes can happen dozens or even hundreds of times every night, and most patients have no memory of them. What the body experiences during each event is anything but harmless:
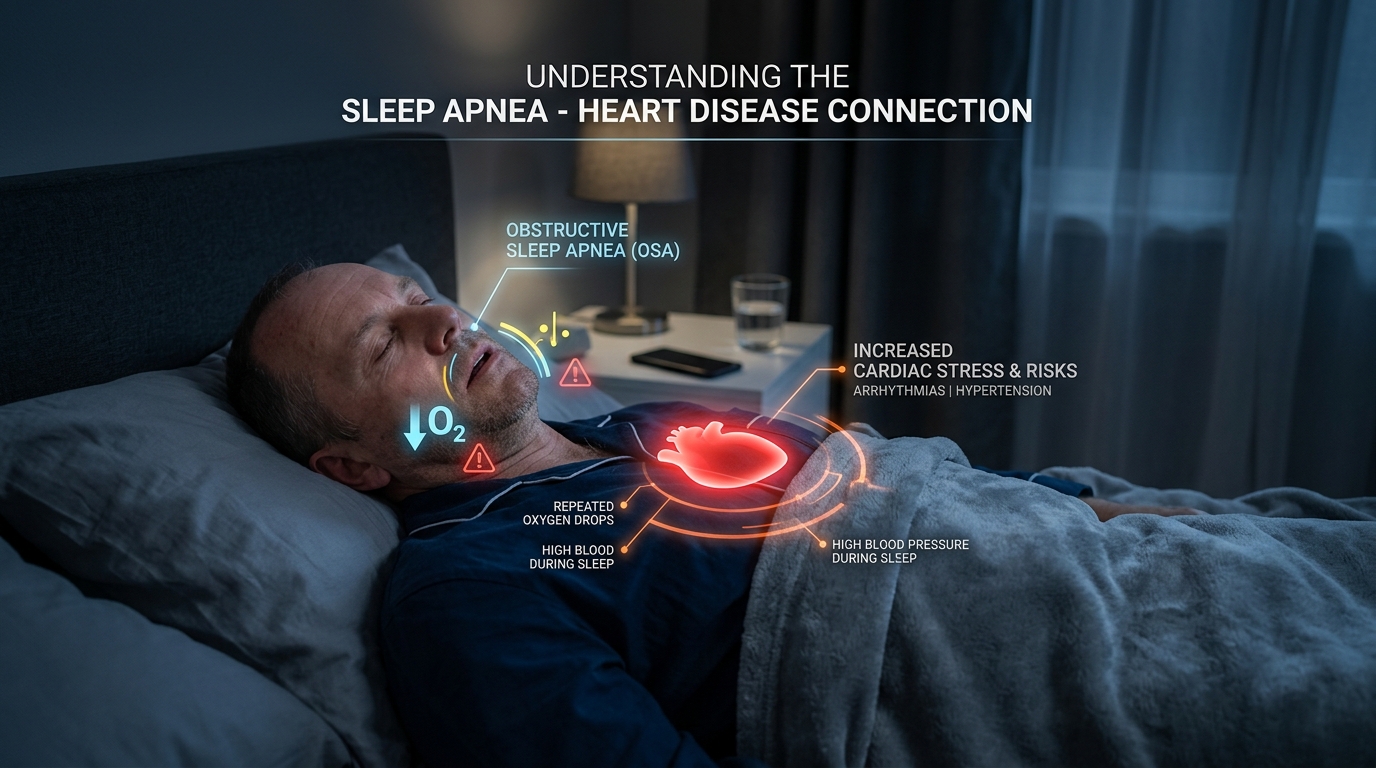
- Drops in blood oxygen levels (intermittent hypoxia).
- Micro-awakenings that fragment sleep without waking the patient consciously.
- Surges of stress hormones (adrenaline, cortisol).
- Spikes in heart rate and blood pressure.
- Cardiovascular and metabolic strain repeated, night after night, for years.
This is why OSA is not just a “snoring problem”—it is a chronic, whole-body stress on the cardiovascular and metabolic system.
Common symptoms of OSA
Night-time symptoms
- Loud habitual snoring, often heard through closed doors.
- Witnessed pauses in breathing (a partner notices breathing stop, then a sudden gasp or snort).
- Choking or gasping during sleep.
- Restless sleep, frequent position changes.
- Frequent night-time urination (nocturia)—often misattributed to prostate or kidney problems.
- Dry mouth or sore throat on waking.
- Sweating during sleep.
Daytime symptoms
- Morning headache, often dull and frontal.
- Daytime sleepiness, especially in passive situations (after lunch, watching TV, in meetings, while driving).
- Poor concentration and memory.
- Irritability, low mood, or short temper.
- Reduced work performance.
- Falling asleep at the wheel or while waiting at traffic signals.
- Reduced libido and intimacy issues.

A patient who needs a strong tea or coffee just to function in the morning, and another after lunch to stay awake, is often describing untreated OSA.
The real-world health risks of untreated OSA
Untreated obstructive sleep apnea is not a quality-of-life issue alone. Strong clinical evidence over decades has linked OSA to multiple systemic risks. The list below is not fearmongering—it is the standard reason every cardiologist, endocrinologist, and ENT surgeon today asks patients about sleep.
1. High blood pressure (hypertension)
Repeated oxygen drops and arousals activate the sympathetic nervous system, leading to:
- Persistent daytime hypertension.
- Resistant hypertension that does not respond well to multiple medications.
- High night-time blood pressure (non-dipping pattern).
OSA is one of the most under-recognised causes of difficult-to-control BP in middle-aged adults.
2. Heart disease
OSA is associated with:
- Coronary artery disease and heart attacks.
- Heart failure (especially diastolic dysfunction).
- Enlargement and remodelling of the heart’s chambers.
- Worse outcomes after cardiac events.
3. Stroke
OSA significantly increases the risk of ischaemic stroke and worsens recovery after one. In any patient with snoring plus hypertension, prior stroke or TIA, obesity, and daytime sleepiness, sleep apnea must be ruled out.
4. Atrial fibrillation and arrhythmias
OSA is strongly linked with:
- Atrial fibrillation (and recurrence after cardioversion or ablation).
- Bradycardias and pauses during sleep.
- Other rhythm disturbances.
5. Type 2 diabetes and insulin resistance
Intermittent oxygen deprivation and fragmented sleep impair glucose metabolism. OSA is associated with insulin resistance, weight gain (which then worsens OSA), and poor diabetes control despite medication adherence.
6. Road traffic and workplace accidents

Daytime drowsiness from untreated OSA is one of the most preventable—and dangerous—public health issues. It increases the risk of:
- Falling asleep while driving, including at signals and on highways.
- Reduced reaction times comparable to driving under alcohol influence.
- Workplace errors in safety-sensitive jobs.
- Industrial and machinery accidents.
This is especially relevant in Kerala, where many patients drive long commutes on busy roads or operate vehicles for a living.
7. Mood, cognition, and depression
Untreated OSA can mimic or worsen:
- Depression and anxiety.
- Brain fog and slowed thinking.
- Memory difficulties.
- In older adults, accelerated cognitive decline.

Many patients started on antidepressants for “fatigue and low mood” actually have untreated OSA underneath.
8. Quality of life and relationships
Snoring routinely disrupts a partner’s sleep, leads to separate bedrooms, and creates ongoing relational strain. Patients themselves often withdraw from social events because they “can’t keep their eyes open after 8 pm”. Treating OSA usually transforms both.
Who is at higher risk of OSA?
- Overweight or obesity, particularly with abdominal weight.
- Large neck circumference (>40 cm in women, >43 cm in men is a useful threshold).
- Male sex, although women—especially after menopause—are increasingly affected.
- Age over 40.
- Nasal obstruction of any cause.
- Alcohol use, especially in the evening.
- Sedative or sleeping medications.
- Family history of snoring or OSA.
- Recessed lower jaw or other facial structural features.
- Hypothyroidism and certain other endocrine conditions.
You can be slim and still have OSA. Anatomy matters as much as weight.
Warning signs that snoring needs evaluation
Book an ENT and sleep evaluation if you have any of the following:
- Loud snoring most nights of the week.
- Witnessed pauses in breathing or gasping during sleep.
- Waking tired despite 7+ hours in bed.
- Morning headaches.
- Sleepiness while driving or stopping the car to nap.
- Difficult-to-control blood pressure, even on multiple medications.
- Diabetes with persistent fatigue despite good sugars.
- Recent weight gain with worsening tiredness.
- Heart attack, stroke, or atrial fibrillation with snoring history.
These are the patterns that turn snoring from a domestic complaint into a medical priority.
Children can have sleep apnea too
Sleep apnea is not only an adult disease. Pediatric OSA is most often caused by:
- Enlarged adenoids.
- Enlarged tonsils.
- Nasal obstruction, including allergy.
Suspect pediatric OSA in a child with:
- Mouth breathing day and night.
- Restless sleep with unusual sleep positions (neck extended, chin up).
- Loud snoring or pauses noted by parents.
- Bedwetting beyond the usual age.
- Poor school focus, hyperactivity-like behaviour.
- Slower growth or low appetite in the morning.
In children, treatment is usually an adenotonsillectomy, often with dramatic improvement in sleep, behaviour, and growth. (See our separate article on mouth breathing and snoring in children for details.)
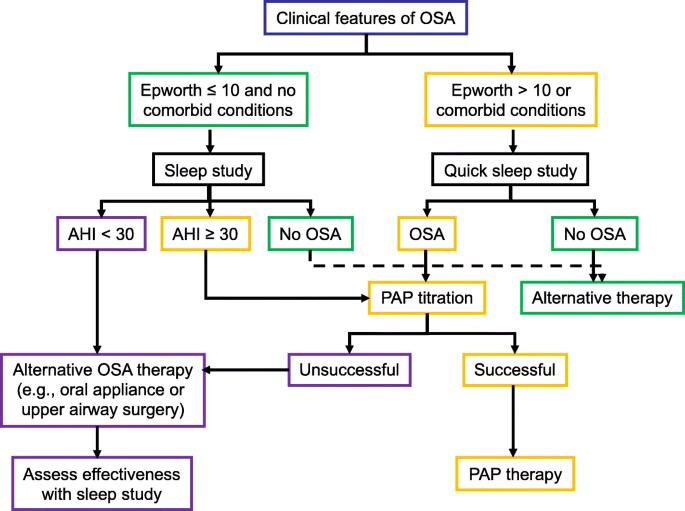
How OSA is diagnosed
Diagnosis at Dr Joel’s Clear ENT Clinic in Thiruvananthapuram is structured to confirm whether OSA is present, how severe it is, and where in the airway the obstruction is happening—because that drives treatment.
A typical evaluation includes:
- Detailed clinical history, including a partner’s account where possible.
- Validated questionnaires (Epworth Sleepiness Scale, STOP-Bang) for risk stratification.
- Full ENT airway examination—nose, oral cavity, oropharynx, tonsils, palate, tongue base.
- Diagnostic nasal endoscopy to assess nasal obstruction and post-nasal anatomy.
- Awake airway assessment (modified Mallampati, palate position, jaw configuration).
- Sleep study — either an in-lab polysomnography or a validated home sleep test, depending on the case. This is the diagnostic gold standard.
- DISE (drug-induced sleep endoscopy) in selected patients being considered for surgery, to identify the exact site(s) of collapse.
Most patients do not need every test. The point is to match the depth of investigation to the severity of the problem.
Treatment of snoring and OSA
There is no single “best” treatment—the right choice depends on severity, anatomy, body weight, comorbidities, and patient preference. A good plan often combines several elements.
1. Lifestyle measures (always)
- Weight reduction — even modest weight loss can significantly reduce severity.
- Avoid alcohol for at least 3 hours before bed.
- Avoid sedatives unless medically necessary.
- Side-sleeping instead of back-sleeping.
- Regular sleep schedule with adequate duration.
- Treat nasal allergies and congestion.
- Smoking cessation.
2. CPAP — the gold standard for moderate to severe OSA
Continuous Positive Airway Pressure delivers a gentle stream of air through a mask, splinting the airway open. When used consistently:
- Snoring stops.
- Oxygen levels normalise.
- Sleep architecture restores.
- Daytime sleepiness, BP, mood, and metabolic markers improve.
Modern CPAP devices are quiet, compact, and well-tolerated when set up properly. Initial mask fitting and follow-up matter—giving up after one bad night is the most common reason patients abandon CPAP unnecessarily.
3. Oral appliances
Mandibular advancement devices reposition the lower jaw and tongue forward during sleep. They are useful for:
- Mild to moderate OSA.
- Primary snoring without significant apnea.
- Patients who cannot tolerate CPAP.
A dental sleep specialist’s involvement is important to avoid jaw-joint and bite issues.
4. ENT and surgical treatment (selected patients)
Surgery is not first-line for everyone, but for carefully selected patients, it can be transformative. Options include:
- Nasal surgery — septoplasty, turbinate reduction, sinus surgery, polyp removal—for patients whose primary issue is nasal obstruction.
- Tonsil and adenoid surgery — especially in younger adults with large tonsils, and the standard treatment in children.
- Palatal procedures — uvulopalatopharyngoplasty (UPPP) and modern variants, for selected palatal-level obstruction.
- Multilevel airway surgery — combining procedures in adults with obstruction at more than one level, often guided by DISE findings.
- Hypoglossal nerve stimulation — an emerging option for selected non-CPAP-tolerant patients.
The single most important rule is correct patient selection: surgery only works when it targets the actual site of obstruction.
Common mistakes seen in real practice
These are gentle observations from years of consulting patients with snoring and OSA—not criticisms:
- Ignoring snoring for years, until a partner refuses to share the bedroom or a cardiac event forces the issue.
- Assuming snoring is normal aging or a “Malayali male thing”.
- Treating only acidity, hypertension, or fatigue while the underlying OSA goes undetected for a decade.
- Buying anti-snoring sprays, mouthpieces, and gadgets online without ever being examined.
- Avoiding a sleep study because it sounds inconvenient or expensive—when in fact it is a one-night, often home-based test.
- Buying a CPAP from the internet without a prescription, fitting, or follow-up, then giving up.
- Stopping CPAP after a few weeks because it “felt strange”, instead of getting the mask and pressure adjusted.
Kerala-specific patterns we see in clinic
Patients in Trivandrum and across Kerala often present late for surprisingly consistent reasons:
- Snoring is normalised in the family—everyone snores, so it is treated as part of life.
- Daytime tiredness is blamed on heat, work stress, or “weakness”, and self-treated with multivitamins.
- BP and diabetes are managed in separate clinics, and OSA—the common factor underneath—is never asked about.
- Sleep studies are postponed for months, even when clearly indicated.
- Patients consult an ENT doctor in Trivandrum only after a cardiac event or after a partner insists.
The encouraging news: when OSA is finally diagnosed and treated, multiple problems often improve at the same time—blood pressure becomes easier to control, sugars settle, mornings feel different, and energy returns.
When to consult an ENT specialist for snoring
Consider an ENT consultation in Thiruvananthapuram if:
- You snore loudly most nights.
- A partner has noticed breathing pauses or gasping.
- You wake up tired despite a full night’s sleep.
- You feel sleepy while driving or in meetings.
- Your blood pressure or diabetes is poorly controlled despite good treatment.
- You have nasal obstruction, large tonsils, or a history of mouth breathing.
- A child in your household snores loudly with restless sleep.
At Dr Joel’s Clear ENT Clinic in Thiruvananthapuram, a snoring evaluation is structured to give you a clear diagnosis, an explanation of severity, and a realistic, individualised plan—whether that is lifestyle, CPAP, an oral appliance, ENT surgery, or a combination.
Key takeaway
Snoring may sound trivial, but loud habitual snoring is one of the most useful warning signs in adult medicine. Behind it often sits obstructive sleep apnea—a condition with proven links to high blood pressure, heart disease, stroke, atrial fibrillation, diabetes, accidents, and a measurably worse quality of life.
The good news is that OSA is diagnosable and treatable, and most patients feel transformed within weeks of starting the right treatment. The first step is simply to take the snoring seriously enough to get it evaluated.
If you or a family member is searching for a sleep apnea specialist or an ENT doctor in Trivandrum for snoring treatment in Thiruvananthapuram, an early, focused consultation is the shortest path from a noisy bedroom to a healthier heart, sharper days, and steadier nights.

