Understanding vertigo in depth: causes, symptoms, diagnosis and treatment
Vertigo is a symptom, not a disease—most often caused by an inner ear balance problem. A clear, ENT-led guide to causes, symptoms, diagnosis, and modern treatment.

If you have ever felt the room suddenly spin when you turned over in bed, or experienced a wave of motion when you tilted your head back, you have probably had a brief encounter with vertigo.
Vertigo is one of the most common—and most misunderstood—symptoms seen in ENT practice. Patients are often told it is “BP”, “gas trouble”, “weakness”, or “spondylosis”, and end up taking long courses of dizziness tablets without ever finding the real cause.
This guide is written from clinical experience at Dr Joel’s Clear ENT Clinic in Thiruvananthapuram, where vertigo is one of the most common reasons patients book a consultation. The aim here is to help you understand vertigo properly: what it actually is, why vertigo happens, the main causes of vertigo, how it is diagnosed, and the modern, evidence-based options for vertigo treatment.
The single most important thing to know is this: vertigo is a symptom, not a disease. Treating it well begins with finding what is causing it.
What is vertigo?
Vertigo is a false sensation of movement. People describe it in different ways:
- The room is spinning around you.
- You feel as if you are moving while standing still.
- The floor seems to tilt or sway.
- A brief “lurch” or “drop” when changing position.
It is not the same as feeling faint, light-headed, or weak. That distinction is critical, because inner ear vertigo has very different causes—and treatments—from light-headedness due to low blood pressure, anaemia, or dehydration.
How balance works (and why vertigo happens)
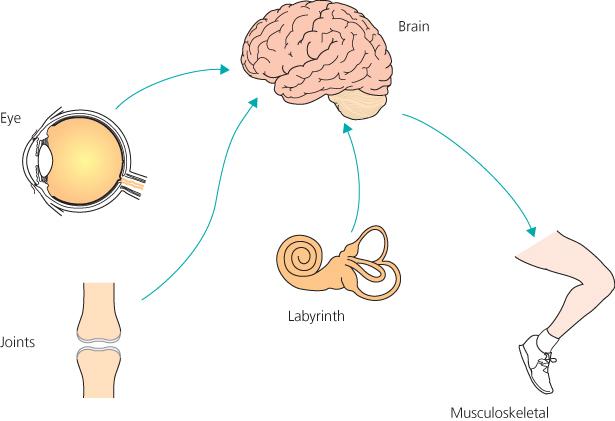
Balance is not controlled by one organ. Your brain continuously combines information from three systems:
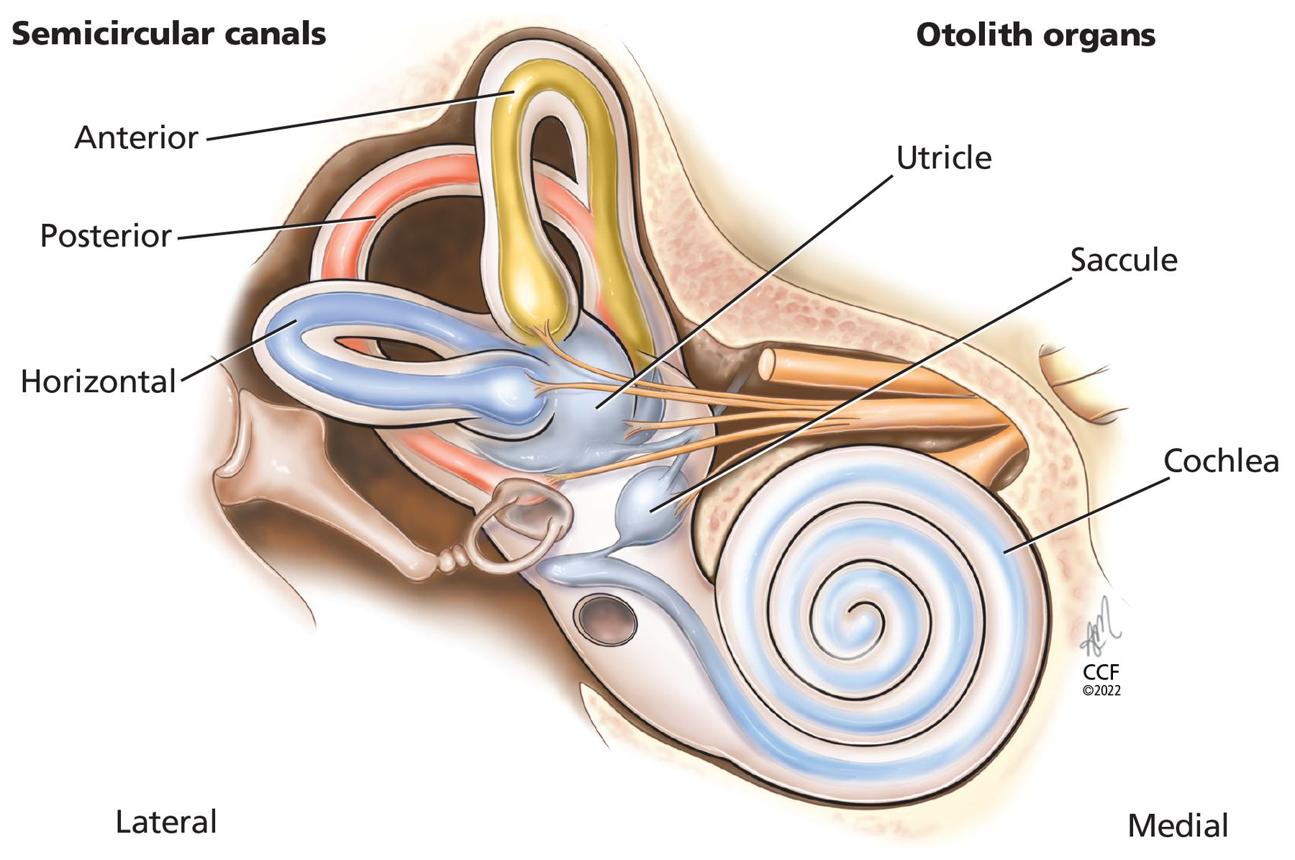
- The inner ear (vestibular system) — fluid-filled canals and otolith organs that detect head movement and gravity.
- The eyes (visual system) — tell the brain where you are in space.
- The body (proprioception) — joints, muscles, and skin send back information about position and movement.
When all three agree, you feel steady. Vertigo happens when these signals disagree. If the inner ear suddenly says “you are spinning” but your eyes and body say “you are still”, the brain experiences a violent mismatch—and that mismatch is felt as spinning, nausea, and imbalance.
Dizziness vs vertigo vs imbalance vs weakness
Patients and even some clinicians use these words interchangeably, but they mean very different things:
- Vertigo — a false sensation of movement, usually spinning. Suggests a vestibular cause.
- Dizziness / light-headedness — feeling faint, “blacking out”, or as if you might pass out. Often related to blood pressure, blood sugar, hydration, or cardiac issues.
- Imbalance / unsteadiness — feeling unsteady on the feet without spinning. Common in elderly patients, neurological disease, or after a vestibular event.
- Weakness — true loss of strength in the limbs. This is a neurological symptom, not vertigo, and needs urgent assessment.
The single best question your ENT will ask you is: “When you have the symptom, does the world spin, or do you just feel you might fall or faint?” The answer alone narrows the diagnosis dramatically.
The main causes of vertigo
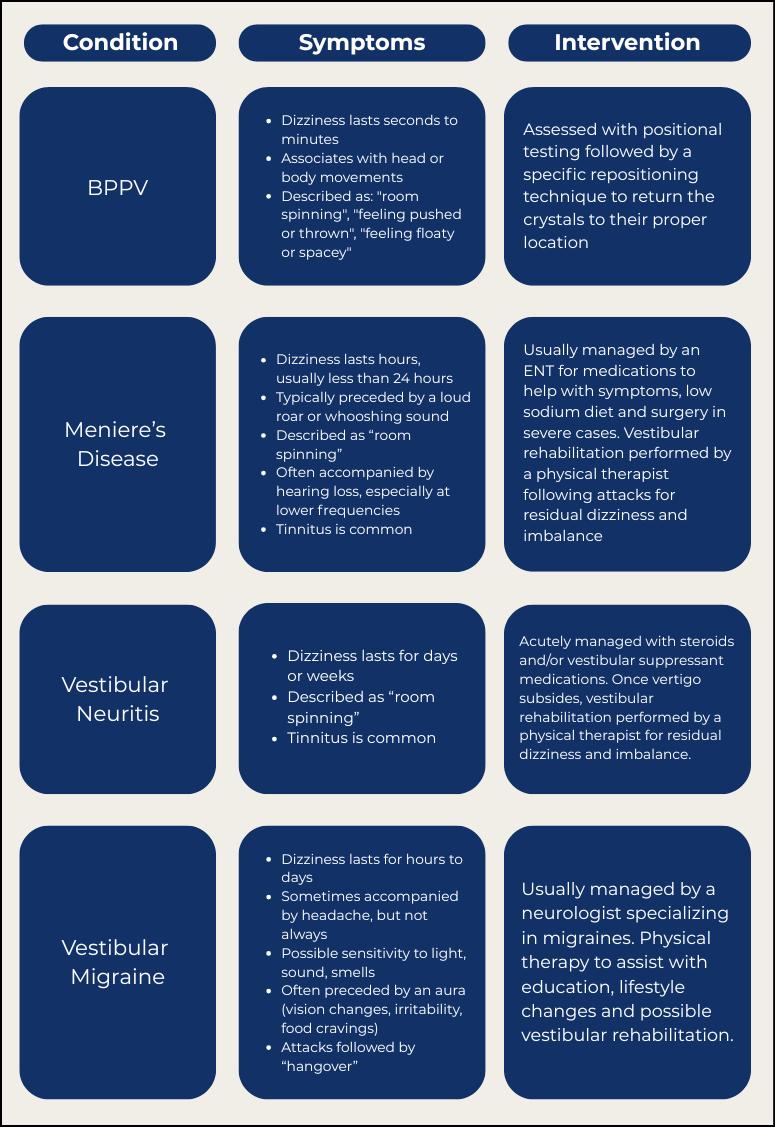
1. BPPV (benign paroxysmal positional vertigo) — the most common cause
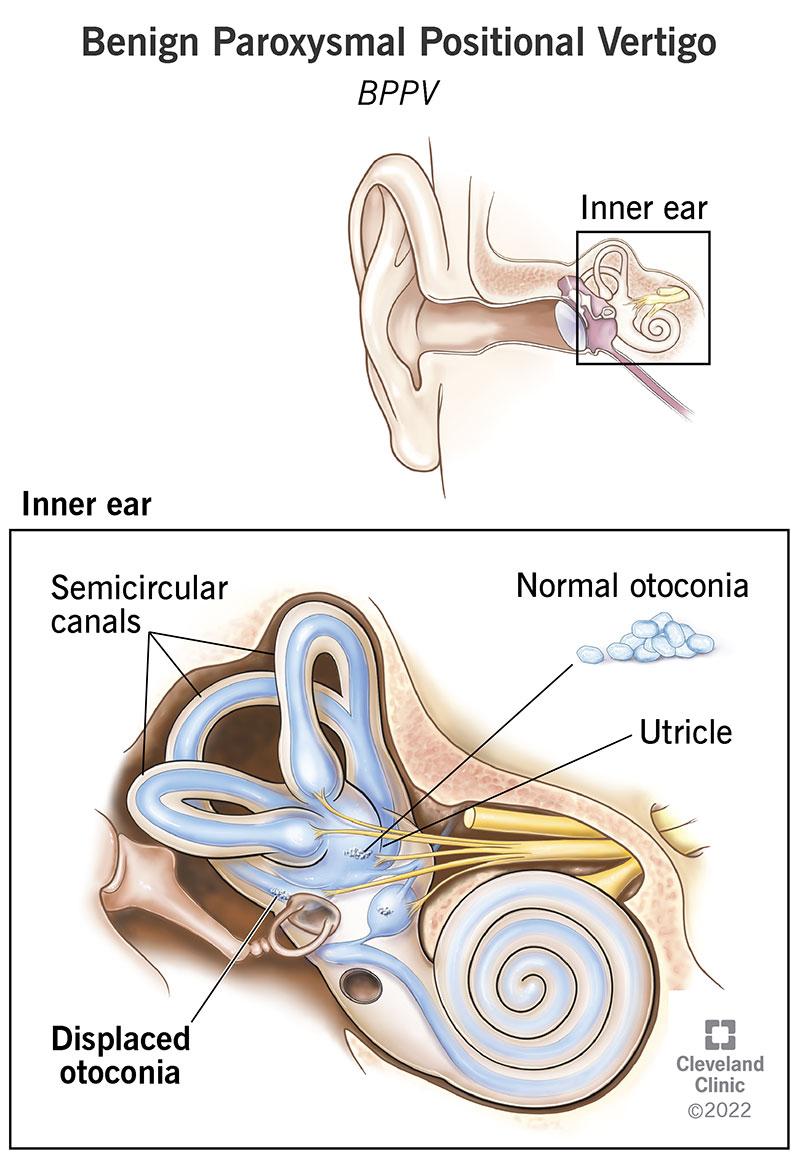
BPPV vertigo accounts for roughly half of all vertigo seen in ENT clinics.
In BPPV, tiny calcium carbonate crystals (otoconia) become displaced from where they belong and fall into one of the semicircular canals of the inner ear. When you move your head, these stray crystals move the fluid in the canal and trick the brain into thinking you are spinning.
Typical features:
- Sudden, brief spinning (seconds to under a minute) triggered by position change.
- Turning over in bed, lying down, getting up, or looking up to a shelf are classic triggers.
- Often associated with nausea, but rarely hearing loss.
- Episodes come and go over days to weeks.
The good news: BPPV is highly treatable. A bedside repositioning manoeuvre (see below) often relieves it in a single visit—this is one of the most satisfying conditions we treat at the clinic, because patients who have suffered for weeks often walk out steady the same day.
2. Vestibular neuritis
Sudden, severe, continuous spinning lasting hours to days, usually after a viral illness. The vestibular nerve becomes inflamed and stops sending balance signals from one ear.
- Hearing is not affected.
- Often accompanied by intense nausea and vomiting.
- Settles gradually as the brain compensates, helped by vestibular rehabilitation.
3. Labyrinthitis
Similar to vestibular neuritis, but inflammation involves the inner ear itself, so hearing loss and tinnitus are also present along with vertigo. Needs prompt ENT assessment because some cases need treatment to protect hearing.
4. Ménière’s disease
A chronic inner ear disorder caused by abnormal fluid pressure (endolymphatic hydrops). The classic pattern is:
- Recurrent attacks of vertigo lasting 20 minutes to several hours.
- Fluctuating hearing loss in one ear.
- Tinnitus (a low-pitched roaring or ringing).
- A sensation of fullness or pressure in the affected ear.
Ménière’s cannot always be cured, but with diet (low salt), specific medications, and sometimes office-based procedures, attacks can be substantially reduced.
5. Vestibular migraine
Often missed for years. Patients have episodes of vertigo or motion sensitivity that may or may not be accompanied by headache. Triggers include sleep deprivation, stress, certain foods, and hormonal changes. Treatment is the same as for migraine itself, not vertigo medications.
6. Anxiety-related dizziness (PPPD)
Persistent postural-perceptual dizziness is a chronic feeling of unsteadiness or “rocking”, often following a true vestibular event. Anxiety amplifies it. This is a real diagnosis with real treatment—vestibular rehabilitation, reassurance, and sometimes specific medication—not just “stress”.
7. Cervical (neck-related) dizziness
Neck pathology can contribute to a feeling of imbalance, especially in older adults with cervical spondylosis, but it is rarely the cause of true spinning vertigo. Many patients in Kerala are told their vertigo is due to “neck”, when the real cause is BPPV in the inner ear—missed because no one performed the simple positional test.
8. Stroke and other central causes (red flag)
A small but important minority of patients with vertigo have a problem in the brainstem or cerebellum, including stroke. Warning features include:
- New severe headache.
- Double vision, slurred speech, or facial weakness.
- Limb weakness or numbness.
- Inability to walk even with help.
- Vertigo that does not change with head position and lasts continuously.
These features mean emergency hospital assessment, not an outpatient ENT appointment.
Why does vertigo happen with position change?
This is the question almost every patient asks: “Why do I get vertigo only when I turn in bed, or when I look up?”
The answer is the inner ear’s anatomy. The semicircular canals are three loops, each oriented in a different plane, that detect rotation. When otoconia crystals dislodge and fall into one of these canals, gravity moves them every time your head changes position relative to gravity.
That is why the classic triggers are:
- Turning over in bed (rotates the head in the canal that lies sideways when you sleep).
- Sitting up suddenly from lying down.
- Bending forward to tie shoelaces or pick something up.
- Looking up at a shelf, hanging clothes, or in a place of worship.
Once the head settles, the crystals stop moving—and the spinning stops within seconds. This pattern is so characteristic that an experienced ENT can often suspect BPPV vertigo from the history alone, before any test.
Why does vertigo cause nausea and vomiting?
Many patients are surprised that an ear problem can make them vomit. The reason is anatomical: the vestibular nuclei in the brainstem sit very close to the vomiting centre, and they share neural connections.
When the balance system fires abnormally, it spills signals into the vomiting centre. Your brain interprets the situation the same way it would interpret motion sickness or food poisoning—and triggers nausea and vomiting as a “protective” response.
This is why anti-nausea medication (like prochlorperazine or ondansetron) often helps a vertigo attack, even though they do nothing for the underlying cause.
How an ENT diagnoses vertigo
Most vertigo can be diagnosed clinically, often within minutes, without expensive scans. At Dr Joel’s Clear ENT Clinic in Thiruvananthapuram, a typical vertigo consultation includes:
1. History (the most important step)
- When did it start, and how long does each episode last? (Seconds, minutes, hours, days?)
- Is it triggered by position change, or does it come at random?
- Is there hearing loss, tinnitus, or ear fullness?
- Is there headache, visual change, weakness, or numbness?
- Any recent viral illness, head injury, or medication change?
2. Bedside examination
- Eye movement examination (looking for nystagmus—involuntary jerking eye movements that betray a vestibular problem and often point to the affected ear).
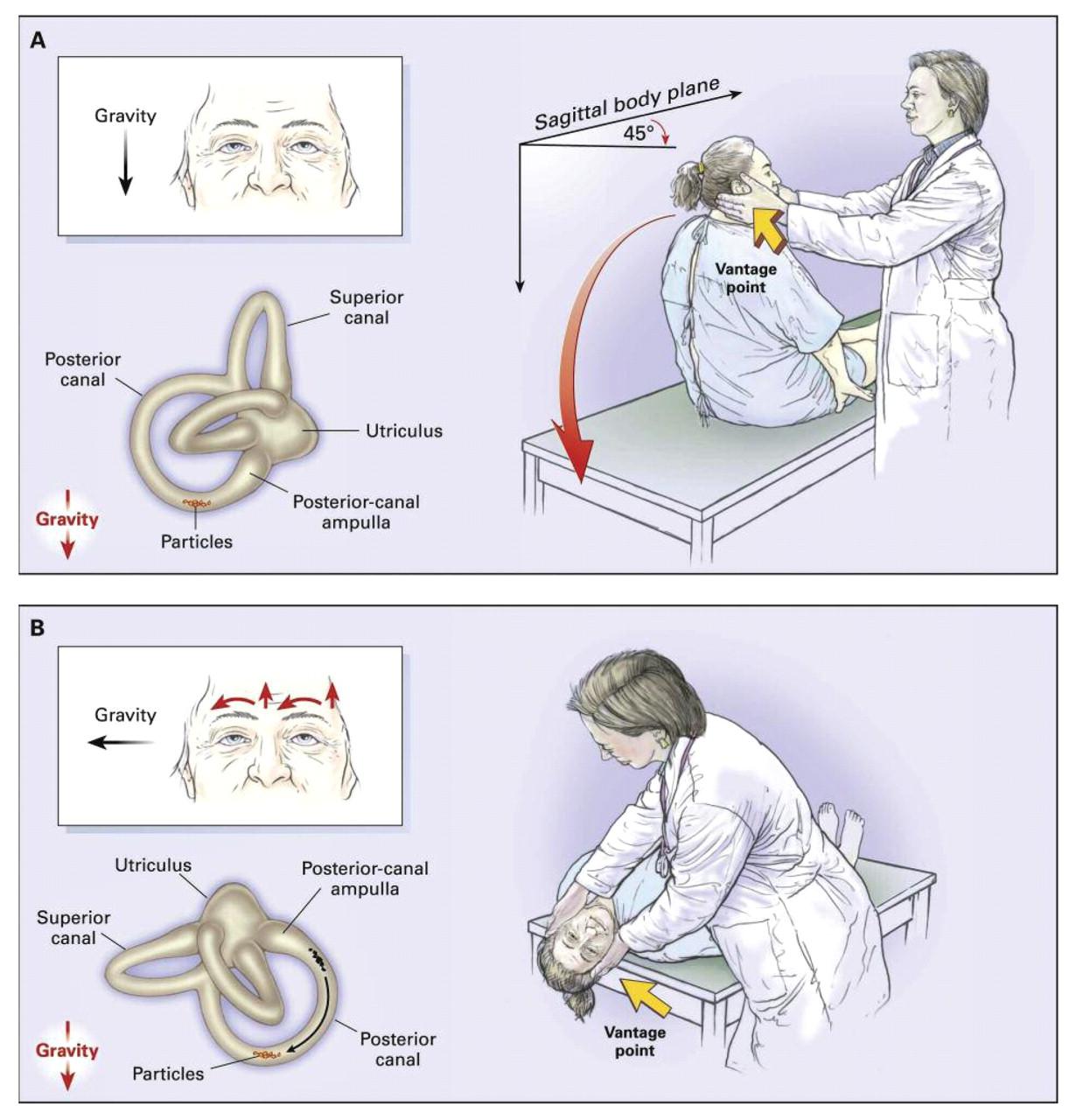
- Dix–Hallpike test — the gold standard bedside test for posterior canal BPPV. The patient is rapidly tilted backwards with the head turned to one side, and the eyes are observed for the characteristic nystagmus.
- Supine roll test for horizontal canal BPPV.
- Head impulse test, gait, and balance assessment to look for vestibular nerve loss or central signs.
3. Hearing test (audiometry)
Useful when Ménière’s, labyrinthitis, or sudden sensorineural hearing loss is suspected.
4. Imaging (only when indicated)
An MRI is helpful when there are red flags pointing to the brain, or when single-sided hearing loss with vertigo raises suspicion of a tumour of the vestibular nerve. Most patients with vertigo do not need a scan. Routine CT or MRI for typical positional vertigo is unnecessary, expensive, and rarely changes treatment.
Modern treatment of vertigo
Treatment depends entirely on the cause—which is exactly why diagnosis matters more than another prescription.
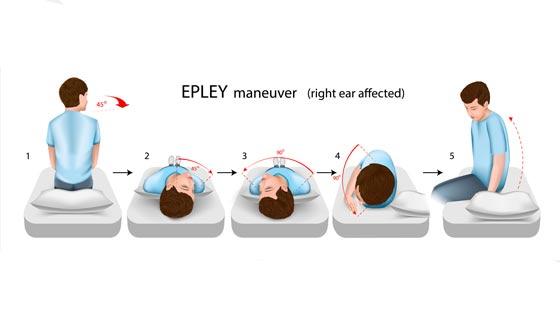
BPPV — repositioning manoeuvres
The Epley manoeuvre (and related canalith repositioning techniques) physically guide the displaced crystals out of the affected semicircular canal and back to where they belong. At the clinic, many patients arrive after weeks of dizziness tablets and walk out significantly better after one session. Repeat sessions or self-administered home exercises (like Brandt–Daroff) are sometimes needed.
Vestibular neuritis and labyrinthitis
- Short-course vestibular suppressants (e.g. prochlorperazine) for the first 24–72 hours only—just enough to control the worst nausea and spinning.
- Early mobilisation and vestibular rehabilitation (specific eye and balance exercises) to help the brain compensate. This is far more important than long-term tablets.
- Steroids may be considered in selected cases.
Ménière’s disease
- Low-salt diet, caffeine and alcohol moderation, good sleep.
- Diuretics and betahistine in many patients.
- Office-based intratympanic injections in resistant cases.
- Surgery for a small minority.
Vestibular migraine
- Identify and avoid triggers (sleep, dehydration, specific foods).
- Migraine-specific preventive medication—not vertigo tablets.
- Lifestyle modification.
A word about long-term “vertigo tablets”
It is very common to see patients in Kerala who have been on cinnarizine, betahistine, or similar tablets for months or years without any clear diagnosis. This is rarely the right approach. These medications:
- Suppress symptoms but do not treat the cause.
- Can actually delay recovery by preventing the brain from compensating.
- May cause side effects, including drowsiness, weight gain, and (in elderly patients) parkinsonism with prolonged use.
Long-term vertigo tablets without a diagnosis are usually wrong. A short course is fine; months of treatment without an explanation is not.
Common mistakes patients make
In Kerala, well-meaning patients often delay proper care because of widespread beliefs about dizziness. The following are gentle observations, not criticisms—we see them every week:
- Assuming all vertigo is “BP” or “gas trouble” and self-medicating from a pharmacy for weeks.
- Putting oil or home remedies in the ear for vertigo. The inner ear is not the ear canal—oil cannot reach it, and the wrong drops can damage an inflamed canal or perforated drum.
- Repeated pharmacy purchases of cinnarizine or stemetil over many months, without ever being examined.
- Jumping straight to MRI for typical positional vertigo, when a 2-minute bedside test would have given the answer.
- Stopping all activity out of fear of falling, which actually slows recovery.
- Delaying ENT consultation until weeks of symptoms have passed.
A single, well-conducted ENT consultation can often resolve in one visit what self-treatment cannot resolve in months.
When is vertigo an emergency?
Most vertigo is not dangerous, but the following features mean you should go to an emergency department, not wait for an ENT appointment:
- Sudden severe headache unlike any before.
- Slurred speech or facial droop.
- Limb weakness or numbness.
- Double vision or new visual loss.
- Inability to walk even with help.
- Loss of consciousness or fainting.
- Sudden hearing loss with vertigo (still urgent, even if only ENT—better hearing recovery if treated early).
These can indicate a stroke, brain bleed, or other neurological emergency where time matters.
How to prepare for your ENT appointment for vertigo
A few minutes of preparation makes the consultation much more useful:
- Note when episodes happen, how long they last, and what triggers them.
- Keep a list of all medications, including over-the-counter dizziness tablets.
- Note any hearing change, tinnitus, or ear fullness.
- Note any headache, visual changes, or neurological symptoms.
- Bring previous scans or audiograms if you have them, but do not get a scan just to bring one.
Conclusion
Vertigo can be frightening, but for most patients it is also one of the most treatable symptoms in ENT practice. The single biggest improvement most patients can make is to stop chasing tablets and start chasing a diagnosis.
To recap:
- Vertigo is a symptom, not a disease.
- The vast majority of vertigo comes from the inner ear balance system, not from BP, neck, or “gas”.
- The most common cause—BPPV—can usually be cured in a single visit.
- Some causes (vestibular neuritis, Ménière’s, vestibular migraine) need a structured plan, not endless tablets.
- A small number of cases are serious and need emergency care; the warning signs above tell you which.
- A clinical, ENT-led assessment is faster, cheaper, and more accurate than scans for most patients.
If you or a family member is searching for an ENT specialist for vertigo, inner ear vertigo treatment, or a dizziness doctor for vertigo treatment in Kerala, an early, focused consultation is almost always the shortest path back to feeling steady. At Dr Joel’s Clear ENT Clinic in Thiruvananthapuram, vertigo is assessed with a careful history, bedside positional testing, and—where indicated—hearing evaluation, with the goal of giving you a clear answer and a definitive plan in a single visit wherever possible.


