Vestibular migraine: the often missed cause of vertigo
Recurrent vertigo that keeps returning despite BPPV treatment, scans, and dizziness tablets may be vestibular migraine—a common but frequently overlooked cause of dizziness, motion sensitivity, and imbalance, often without severe headache.

A patient walks into the clinic complaining of recurrent vertigo. They have already been treated for BPPV, undergone multiple scans, taken medications for “ear imbalance,” and perhaps even been told it is stress or anxiety.
Yet the attacks keep returning.
In many such patients, the true diagnosis is vestibular migraine—one of the most common causes of recurrent vertigo and dizziness, yet one of the most frequently overlooked.
Unlike classic migraine, vestibular migraine does not always present with severe headache. Some patients experience repeated episodes of dizziness, imbalance, motion sensitivity, or vertigo with little or no headache at all.
This guide is written from clinical experience at Dr Joel’s Clear ENT Clinic in Thiruvananthapuram (Trivandrum). It explains what vestibular migraine is, why it is so often missed, how it differs from BPPV and Ménière’s disease, and what evidence-based treatment looks like.
The key idea: If vertigo keeps coming back despite “inner ear” treatment, the diagnosis may not be in the ear at all—it may be migraine affecting the brain’s balance networks.
What is vestibular migraine?
Vestibular migraine is a neurological condition in which migraine mechanisms affect the body’s balance system.
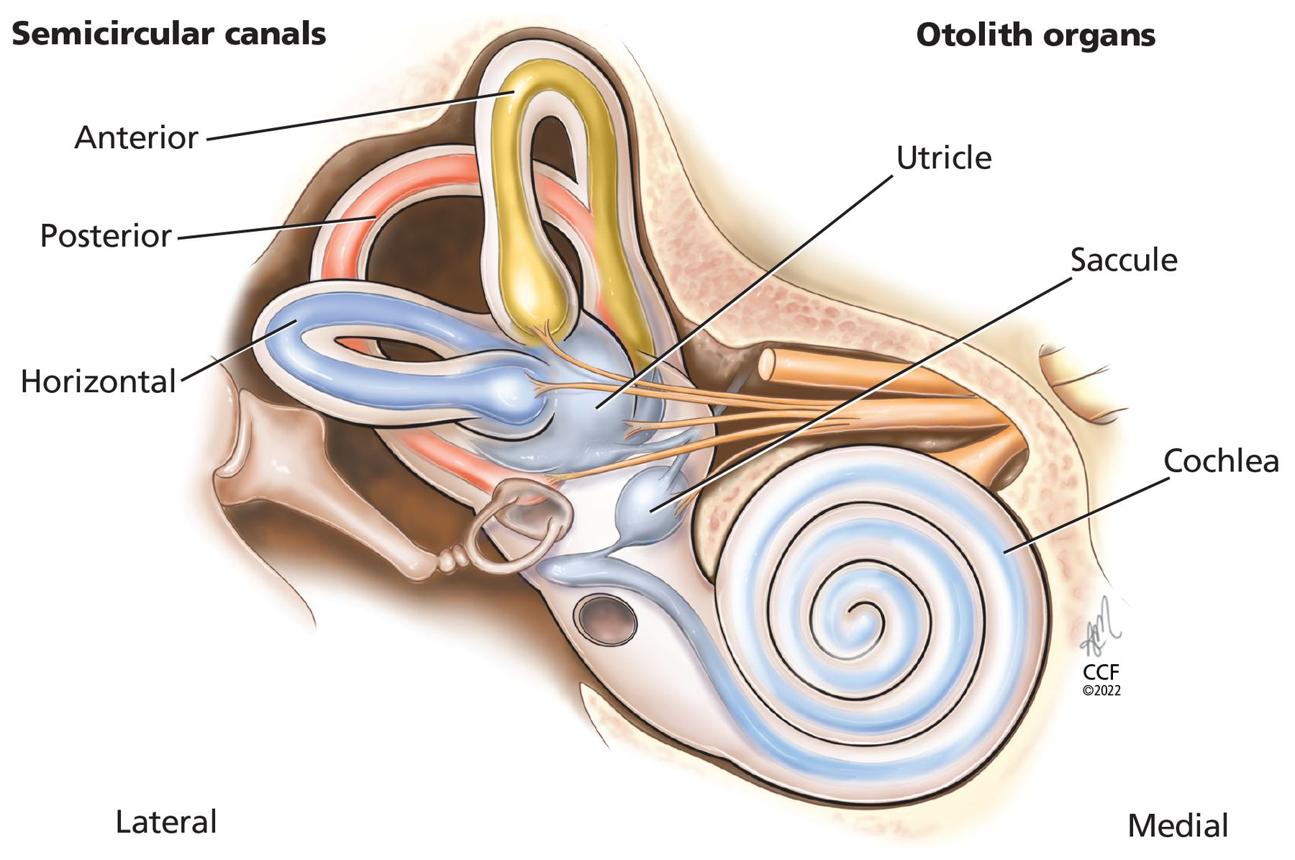
The word vestibular refers to the balance organs of the inner ear and the brain pathways that process balance information. In vestibular migraine, migraine-related activation disrupts how the brain integrates:
- Inner ear balance signals
- Vision
- Motion perception
- Spatial awareness
Instead of causing headache alone, migraine can produce:
- Vertigo (spinning or movement sensation)
- Dizziness and light-headedness
- Motion sensitivity
- Imbalance and unsteadiness
- Visual motion intolerance (busy environments feel overwhelming)
- Sensitivity to head movement
Today, vestibular migraine is recognised as one of the most common causes of recurrent spontaneous vertigo—especially in patients who have been through multiple rounds of treatment without lasting relief.
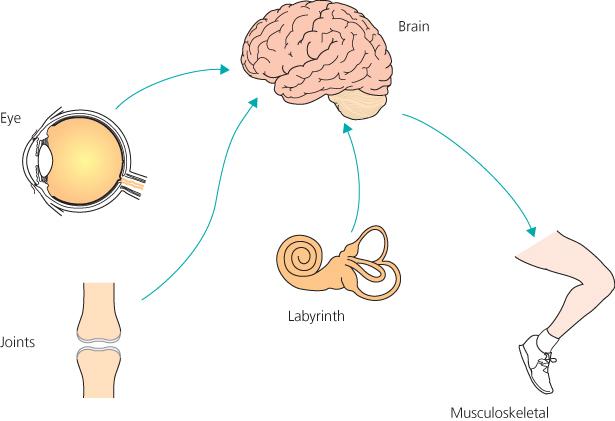
The diagram above illustrates why vestibular migraine feels so “physical”: balance depends on the brain combining signals from the eyes, inner ear, and body. When migraine disrupts that integration, patients feel genuinely dizzy—even when standard ear tests are normal.
Why is vestibular migraine often missed?
Many people—including healthcare professionals—still associate migraine exclusively with headache.
However, vestibular migraine may occur:
- Before a headache
- During a headache
- After a headache
- Completely independent of headache
As a result, patients are often diagnosed with:
- Recurrent BPPV
- Anxiety-related dizziness
- Cervical vertigo (“neck spondylosis”)
- “Weakness”
- “Gas trouble”
- Unexplained dizziness
—before vestibular migraine is considered.
Clinical insight from practice: a common pattern is a patient who has had three or four Epley manoeuvres, multiple normal CT/MRI scans, and months of betahistine or cinnarizine—yet still reports unpredictable attacks in crowded places, during travel, or after poor sleep. That pattern should raise suspicion for vestibular migraine, not another round of positional treatment.
Related reading:
- Understanding vertigo in depth: causes, symptoms, diagnosis and treatment
- Vertigo treatment in Thiruvananthapuram: when to see an ENT doctor
What does vestibular migraine feel like?
Patients describe symptoms very differently—and that variability is part of why the diagnosis is missed.
Some report:
- “The room suddenly starts spinning.”
Others say:
- “I feel as though I’m walking on a boat.”
Or:
- “Crowded places and moving traffic make me dizzy.”
Vertigo
The most frequent symptom. Patients may experience:
- Spinning sensation
- Tilting or rocking sensation
- Feeling pulled to one side
- Sudden “drop” or lurch sensations
Motion sensitivity
Many patients become unusually sensitive to movement. Examples include:
- Travelling in a car or bus
- Watching fast-moving objects
- Scrolling on a phone
- Walking through shopping malls
- Watching action movies
Visual vertigo (visual motion intolerance)
Busy visual environments can trigger symptoms:
- Supermarkets and malls
- Crowded roads
- Escalators
- Large screens
- Moving crowds

Imbalance without spinning
Some patients do not experience classic spinning at all. Instead they describe:
- Unsteadiness or swaying
- Feeling disconnected from the ground
- Difficulty walking in crowded places
- Needing to hold onto walls or furniture
Image suggestion: Simple infographic contrasting “spinning vertigo” vs “rocking imbalance” vs “visual dizziness in busy environments.”
Does headache always occur?
No. This is one of the biggest misconceptions.
Many patients with vestibular migraine have:
- A previous history of migraine
- Family history of migraine
- Childhood motion sickness
—but may not experience severe headache during every attack.
When headache does occur, it often has typical migraine features:
- Throbbing pain
- One-sided headache
- Light sensitivity (photophobia)
- Sound sensitivity (phonophobia)
- Visual aura (in some patients)
- Nausea
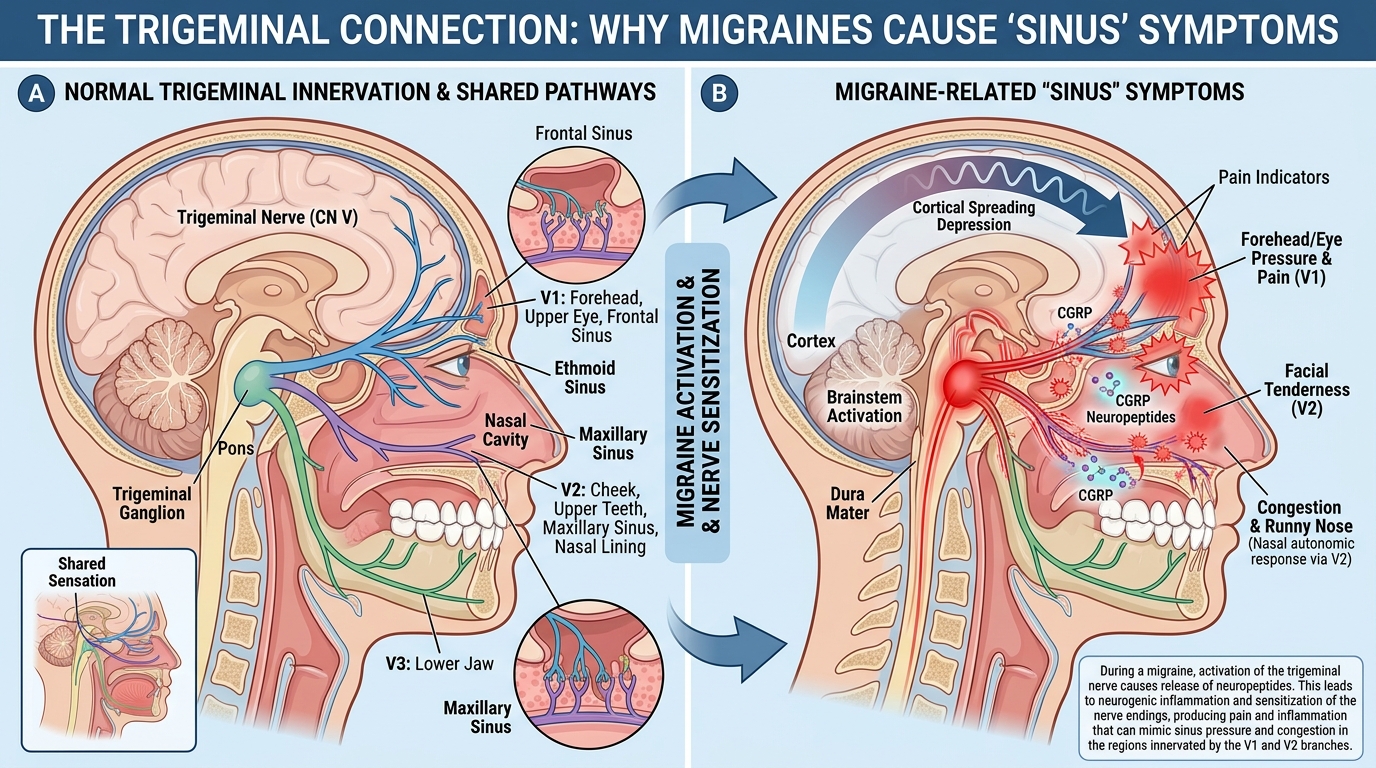
There is overlap with how migraine can mimic sinus disease—facial pressure and nasal symptoms can occur in migraine too. For headache-focused confusion, see:

Why does vestibular migraine happen?
The exact mechanism remains incompletely understood, but current research suggests migraine affects the brain networks that integrate vision, balance, motion perception, and spatial awareness.
Migraine-related activation of nerve pathways may alter communication between:
- Inner ear balance organs
- Brainstem vestibular centres
- Thalamus
- Visual processing centres
This helps explain why patients develop motion sensitivity, visual dizziness, vertigo, and light sensitivity as part of the same condition—not as unrelated problems.
Common triggers
Like traditional migraine, vestibular migraine often has identifiable triggers.
Poor sleep
One of the strongest triggers. Even a single night of inadequate sleep may provoke symptoms.
Stress
Many patients notice attacks during work pressure, emotional stress, examination periods, or major life events.
Skipping meals
Long gaps without food can activate migraine pathways.
Hormonal changes
Particularly around menstruation.
Alcohol
Especially red wine, beer, or excess alcohol intake.
Weather changes
Some patients are sensitive to sudden pressure changes, monsoon weather shifts, or storm systems—common in Kerala’s climate.
How is vestibular migraine different from BPPV?
This is one of the most important distinctions in ENT practice.
BPPV (benign paroxysmal positional vertigo)
Usually:
- Triggered by specific head positions (turning in bed, looking up, bending down)
- Lasts seconds
- Associated with positional nystagmus on examination
- Often responds to repositioning manoeuvres (Epley, etc.)
Vestibular migraine
Usually:
- More variable in timing and trigger
- Lasts minutes to hours, sometimes longer
- May be associated with migraine features (headache, light/sound sensitivity, visual intolerance)
- Not reliably cured by positional manoeuvres alone
Many vestibular migraine patients are repeatedly treated for BPPV before the diagnosis becomes clear.
For a deeper comparison of vertigo causes and bedside testing, see:
Vestibular migraine vs Ménière’s disease
These conditions can appear remarkably similar. Both may cause:
- Vertigo
- Ear fullness
- Tinnitus
However:
Ménière’s disease
Often includes:
- Fluctuating hearing loss documented on audiometry
- Progressive or recurring ear symptoms in a characteristic pattern
- Episodes often lasting 20 minutes to several hours
Vestibular migraine
Usually:
- Hearing remains normal on testing between attacks
- Auditory symptoms (fullness, tinnitus) may be temporary during attacks
- Migraine features (headache, photophobia, visual intolerance) are more prominent
In some patients, distinguishing the two requires repeated evaluations over time—including hearing tests during and between attacks.
Can vestibular migraine cause ear symptoms?
Yes. Many patients report:
- Ear pressure or fullness
- Ringing in the ears (tinnitus)
- Subjective hearing fluctuation
This sometimes leads patients to believe they have an ear infection or blocked ear. Unlike Ménière’s disease, however, hearing usually remains normal between attacks on formal audiometry.
If ear fullness is your main concern alongside dizziness, an ENT examination and hearing test remain important—not to “prove” an ear infection, but to separate Ménière’s, Eustachian tube dysfunction, and vestibular migraine.
How is vestibular migraine diagnosed?
There is currently no blood test, scan, or hearing test that confirms vestibular migraine on its own.
Diagnosis is largely clinical. An ENT specialist or neurologist evaluates:
- Nature and duration of dizziness/vertigo
- Trigger patterns (sleep, stress, visual environments, travel)
- Migraine history (personal and family)
- Associated symptoms (headache, photophobia, nausea)
- Response to previous treatments (BPPV manoeuvres, dizziness tablets, antibiotics)
Investigations may still be needed
Testing is often useful to:
- Exclude Ménière’s disease
- Exclude vestibular neuritis or labyrinthitis
- Evaluate hearing
- Rule out other neurological conditions when the history warrants it
Possible tests include:
- Audiometry (hearing test)
- Vestibular testing (selected cases)
- MRI in selected patients (atypical features, neurological signs, or when another diagnosis needs exclusion)
Important: Normal investigations do not rule out vestibular migraine. In fact, normal scans with recurrent vertigo are sometimes a clue that the problem is functional-disorder migraine pathways rather than structural ear disease.

Important warning: not every vertigo with headache is migraine
This is especially important during a first episode or when symptoms are sudden and severe.
Vertigo associated with:
- Sudden severe “worst headache of life”
- Double vision
- Weakness or numbness
- Slurred speech
- Difficulty walking even with support
- Altered consciousness
requires urgent medical assessment. Serious conditions such as stroke can sometimes mimic vestibular migraine.
If these features are present, go to an emergency department—not an outpatient appointment.
Treatment of vestibular migraine
Treatment usually involves a combination of trigger management, migraine-directed therapy, and—when needed—vestibular rehabilitation. Long-term “vertigo tablets” without a diagnosis are rarely the right answer.
Trigger management
Patients often improve substantially when triggers are addressed:
- Regular sleep schedule
- Adequate hydration
- Consistent meal timing
- Stress reduction strategies
- Moderation of alcohol
- Identifying personal food or weather triggers
Migraine preventive therapy
For frequent or disabling attacks, preventive medications may be considered. Options are individualised and may include medications commonly used for migraine prevention, such as:
- Beta blockers
- Calcium channel blockers
- Certain anti-seizure medications
- Other migraine preventive agents
The choice depends on age, other medical conditions, side-effect profile, and whether headache is a prominent feature.
Newer migraine therapies
Recent advances targeting CGRP (calcitonin gene-related peptide) pathways have expanded options for migraine prevention. Research in vestibular migraine is ongoing, but some patients may benefit from these approaches under specialist guidance.
Vestibular rehabilitation therapy
Vestibular rehabilitation can be particularly helpful for:
- Motion intolerance
- Visual vertigo
- Persistent imbalance
- Activity avoidance (avoiding malls, travel, or driving)
Results tend to be best when migraine control is optimised at the same time—rehabilitation alone, while migraine remains active, often disappoints.
A word about long-term dizziness tablets
It is very common in Kerala to see patients on cinnarizine, betahistine, or similar medications for months or years without a clear diagnosis. For vestibular migraine, this approach often fails because:
- The medication suppresses symptoms without treating migraine pathways
- Prolonged vestibular suppressants can delay compensation
- Side effects (drowsiness, weight gain, parkinsonism in elderly patients) accumulate over time
Short-term symptom control may be reasonable during a severe attack. Long-term treatment should target the underlying migraine mechanism.
Anxiety and vestibular migraine
Many patients develop anxiety because of unpredictable attacks. Others begin avoiding:
- Travel
- Shopping malls
- Social events
- Driving
Persistent dizziness itself can increase anxiety, creating a cycle that worsens symptoms.
Recognising and treating both aspects often improves outcomes. This does not mean “it’s all in your head”—it means vertigo is frightening, and fear naturally amplifies imbalance. Treating vestibular migraine directly often settles the anxiety more effectively than reassurance alone.
Common misconceptions seen in Kerala
In day-to-day practice, patients with vestibular migraine are frequently told their symptoms are due to:
- Gas trouble
- Cervical spondylosis
- Weakness or vitamin deficiency alone
- Ear infection
- Stress alone
While these conditions can sometimes contribute to dizziness, recurrent episodes of vertigo with migraine features deserve proper evaluation.
Another common pattern is repeated treatment with dizziness tablets for months or years without identifying the underlying cause—especially when attacks are triggered by sleep deprivation, visual environments, or travel rather than head position.
When should you see an ENT specialist?
Consider evaluation if you have:
- Recurrent vertigo or dizziness episodes
- Dizziness associated with headache, light sensitivity, or visual intolerance
- Motion sensitivity (cars, malls, screens)
- Visual motion intolerance in busy environments
- Ear fullness with normal hearing tests
- Repeated “unexplained” dizziness episodes
- Vertigo that keeps returning despite BPPV treatment or scans
Early, accurate diagnosis often prevents years of unnecessary investigations and ineffective medication.
For broader guidance on when ENT evaluation is appropriate, see:
- ENT specialist (otolaryngologist): what they treat and when to see an ENT doctor
- When should you see an ENT specialist? Symptoms you should not ignore
Frequently asked questions
Q: Can vestibular migraine occur without headache?
A: Yes. Many patients experience vertigo attacks without significant headache. A history of migraine, family history, or typical migraine features during some attacks supports the diagnosis.
Q: Is vestibular migraine an inner ear disease?
A: Not exactly. It is a migraine-related disorder involving the brain’s processing of balance information, although inner ear pathways may be affected.
Q: Can vestibular migraine be cured?
A: Many patients achieve excellent control with trigger management, lifestyle modification, and appropriate treatment. Symptoms may recur over time, but attacks can become far less frequent and disabling.
Q: Is MRI necessary?
A: Not always. MRI is usually reserved for atypical symptoms, first presentations with neurological warning signs, or when another diagnosis needs exclusion.
Q: Can vestibular migraine cause tinnitus?
A: Yes. Some patients experience tinnitus, ear pressure, or temporary auditory symptoms during attacks. Hearing usually remains normal between episodes on testing.
Q: How is vestibular migraine different from BPPV?
A: BPPV is position-triggered, lasts seconds, and often responds to repositioning manoeuvres. Vestibular migraine is more variable, lasts longer, and is treated with migraine-directed strategies—not repeated Epley manoeuvres alone.
Key takeaway
Vestibular migraine is one of the most common causes of recurrent vertigo, yet it remains underrecognised. Because dizziness may occur without headache, many patients spend years searching for answers—treated repeatedly for BPPV, given normal scans, and left on long-term dizziness tablets—before the diagnosis is considered.
If you experience repeated episodes of vertigo, motion sensitivity, visual dizziness, or unexplained imbalance—especially if you have a personal or family history of migraine—vestibular migraine should be part of the discussion.
Accurate diagnosis is often the first step toward effective treatment and a significant improvement in quality of life.
This article is educational and not a substitute for personalised medical advice. Sudden severe vertigo with neurological symptoms requires emergency assessment.


